Start learning
The text provides an extensive exploration into the anatomical and functional aspects of the lower leg's skeletal structure, focusing on the tibia and fibula, their comparative anatomy, joint articulations, ligament attachments, and clinical relevance. It highlights the tibia as the second longest bone in the human body, essential for weight-bearing and movement, featuring an S-shaped curvature for structural integrity and distributing stresses. The tibia's proximal and distal ends form critical joints at the knee and ankle, respectively, while the fibula, though not primarily a weight-bearing bone, stabilizes the ankle and supports lower leg muscles.
Comparative analysis reveals similarities between the leg's and forearm's bone arrangements, showcasing evolutionary and functional parallels. The text delves into the joint articulations, emphasizing the tibiofemoral and tibiofibular syndesmosis and their importance in the lower limb's stability and function. Crucial ligament attachments to these bones, like the anterior and posterior cruciate ligaments in the knee and the attachments for peroneal muscles on the fibula, underscore their role in movement and stability.
Clinical insights address the commonality of medial and lateral malleolus fractures, their diagnosis, treatment strategies, and the importance of understanding nerve injury implications, such as the common peroneal nerve damage. The detailed examination of the calf's skeletal structures culminates in emphasizing the interplay between the anatomical knowledge of the tibia and fibula with their biomechanical roles in supporting body weight, enabling movement, and contributing to stability. Appendices include a glossary and review questions to further aid in the consolidation of knowledge for medical students, highlighting the significance of the lower leg in medical practice and treatment methodologies.
In our exploration of the human body's remarkable framework, we venture into one of the pivotal regions that exemplify the integration of form, function, and evolution: the lower leg. This area, encompassing the tibia and fibula, serves as a fundamental pillar in understanding not only the skeletal system but also the broader principles of biomechanics and anatomical synergy.
The lower leg is comprised of two primary bones: the tibia and the fibula, which collaborate intricately to support and mobilize the human body. The tibia, known for its robust structure, is the second longest bone in the human body. Its strategic positioning and design are crucial for weight-bearing and distribution, as well as for forming vital joints at the knee and ankle. The bone's superior end articulates with the femur to form the knee joint, while its inferior aspect interacts with the talus at the ankle joint, facilitating a wide range of leg movements.
The fibula, although slender and not directly involved in weight-bearing, plays a vital role in stabilizing the lateral aspect of the ankle and providing attachment points for muscles that control foot dynamics. Its relationship with the tibia, characterized by the interosseous membrane and syndesmosis joint, exemplifies the intricate cooperation between skeletal components.
The comparison between the bones of the lower leg and those of the forearm (the radius and ulna) reveals profound insights into the evolutionary and functional parallels within the human body. Both regions consist of two longitudinal bones that articulate with each other and with their respective proximal and distal joints. In the forearm, the radius and ulna facilitate complex wrist and elbow movements, akin to the tibia and fibula's role in enabling ankle and knee mobility.
What's particularly intriguing is the similarity in the configurational relationship, where one bone (tibia in the leg, ulna in the forearm) is primarily responsible for load-bearing, while the other (fibula in the leg, radius in the forearm) significantly contributes to the range of motion and stabilization. This duality of function is a testament to the body's evolutionary ingenuity, optimizing structures for both strength and flexibility.
Furthermore, the presence of an interosseous membrane in both regions exemplifies a shared architectural strategy, enhancing the cohesion and force distribution between the neighboring bones. Such comparative anatomy not only enriches our understanding of the skeletal system's complexity but also underlines the interconnectedness of human physiology. Through this lens, we appreciate how evolution has sculpted mechanisms that adeptly balance rigidity and mobility, ensuring the organism's survival and functional proficiency.
In conclusion, the study of the lower leg's skeletal anatomy not only provides a window into the marvels of human design but also bridges various concepts in anatomy, biomechanics, and evolution, setting the stage for deeper exploration into the musculoskeletal system's nuances.
The tibia, commonly referred to as the shinbone, is a key structure in the lower leg, playing a crucial role in weight bearing and movement.
The tibia exhibits an S-shaped curvature when viewed from the side. This unique shape provides enhanced structural integrity and resilience under the load of body weight. The superior part of the tibia has a convex medial curvature, which transitions into a concave medial curvature inferiorly. This curvature is not just a structural feature; it plays an essential role in distributing the stresses placed on the lower leg during various activities.
Cross-sectionally, the tibia's body resembles a triangular prism. This shape is characterized by three faces—medial, lateral, and posterior—and three edges—anterior, medial, and interosseous/lateral. The prism-like shape contributes to the bone's strength and provides surfaces for the attachment of muscles and ligaments, further illustrating the tibia's importance in both support and locomotion.
The medial face of the tibia is notable for its flatness and subcutaneous position, making it easily palpable. This surface is important for the attachment of structures like the pes anserinus in its upper part, emphasizing the tibia's role in the musculoskeletal system.
In contrast, the lateral face serves a distinct purpose by accommodating the tibialis anterior muscle along a longitudinal groove in its superior portion. The transformation of this face to become anterior in the lower portion of the tibia is a noteworthy anatomical feature.
The posterior face houses the soleal line, crucial for the attachment of the soleus muscle. This face also features insertion points for the popliteus muscle and serves as the location for the nutrient foramen, highlighting the tibia's nutritional and functional importance.
The anterior edge, or tibial crest, is a prominent feature running along the length of the tibia, ending in the medial malleolus distally. Its palpability and sharpness make it a significant landmark, especially in clinical assessments.
This edge is crucial for the attachment of the interosseous membrane, a fibrous sheet that plays a key role in stabilizing the tibia and fibula and in compartmentalizing the leg muscles.
Condyles and Their Articular Surfaces
The proximal epiphysis of the tibia features two condyles, medial and lateral, each providing an articular surface for the femoral condyles. These surfaces play a crucial role in knee joint stability and mobility, with the medial surface being oval and deeper than the lateral, which is broader in the transverse direction.
Intercondylar Features
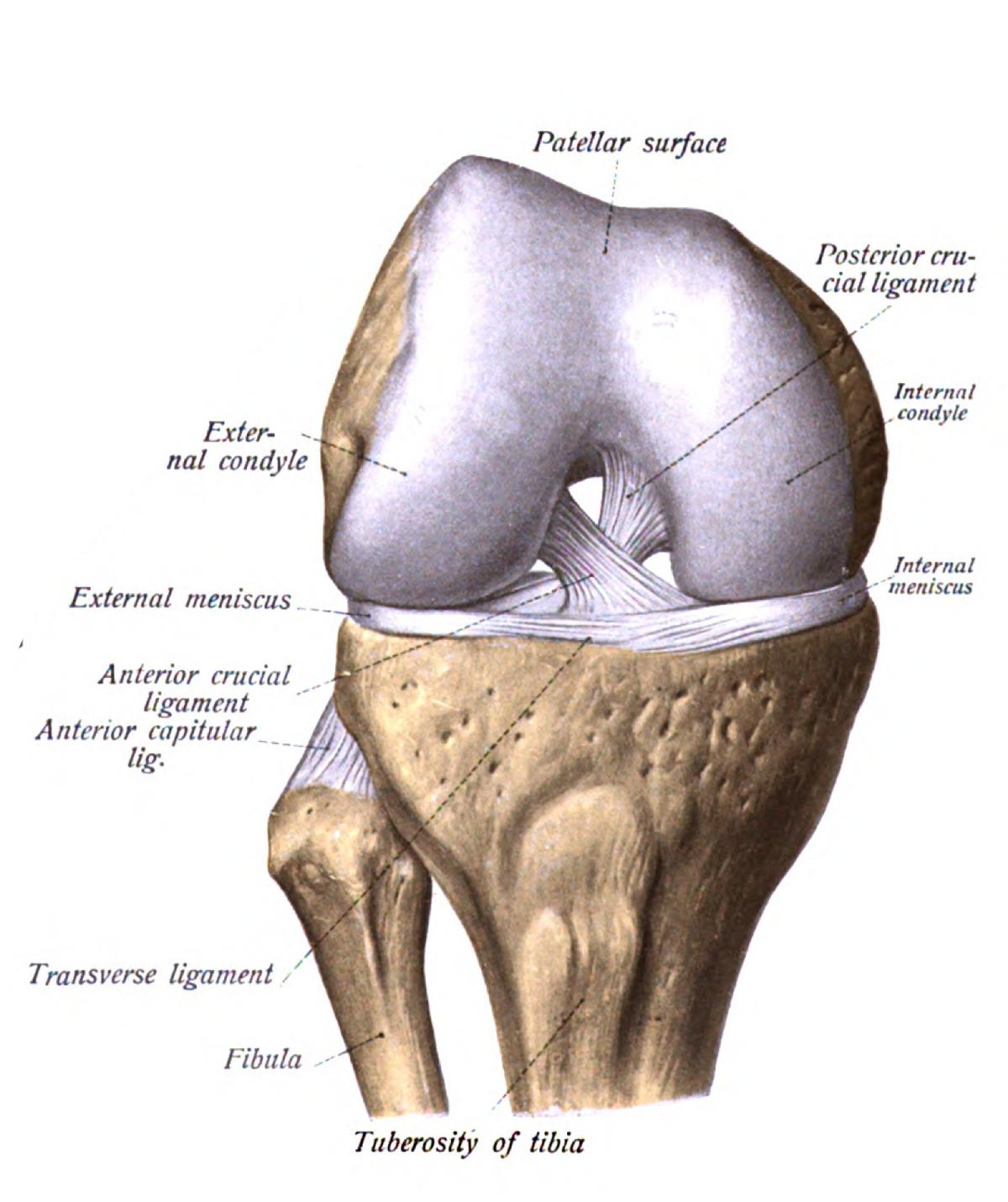
The intercondylar eminence, consisting of two tubercles and a small intervening notch, is pivotal for ligament attachment, notably the anterior and posterior cruciate ligaments. These structures are fundamental to the knee joint's stability, underscoring the tibia's integral role in joint mechanics.
Articulation with the Talus
The distal epiphysis features an inferior articular surface divided by an anteroposterior crest into two facets, accommodating the trochlea of the talus. This articulation is essential for ankle joint mobility, influencing both dorsiflexion and plantarflexion movements.
The Medial Malleolus
The medial malleolus, an extension of the distal tibia, plays an important role in ankle joint stability. This prominence is not only palpable but also prone to fractures, which underscores its clinical significance. Its articular surface with the talus and its role in providing attachment points for ligaments highlight its importance in the anatomical and functional integrity of the ankle joint.
The fibula is a slender, long bone located lateral to the tibia in the lower leg. It plays a crucial role in stabilizing the ankle and supporting muscles of the lower leg, despite not bearing significant body weight. Its structure is characterized by a diaphysis (body) and two epiphyses (ends), with the lateral malleolus forming its distal extremity. The fibula's primary function includes muscle attachment and forming the lateral aspect of the ankle joint, contributing to the lower limb's stability and movement.
The fibula presents three distinct surfaces: lateral, medial, and posterior. The lateral surface serves primarily as the insertion site for the peroneal muscles, crucial for foot eversion and plantarflexion. The medial surface, facing the tibia, is marked by the interosseous membrane attachment, serving as a key site for force transmission between the tibia and fibula. The posterior surface accommodates the attachment of muscles responsible for foot flexion, notably contributing to the plantarflexion motion.
These edges of the fibula define its triangular cross-sectional shape. The anterior edge is relatively smooth and rounded, transitioning between the medial and lateral surfaces. The posterior edge is more pronounced, providing attachment points for the tibia. The interosseous edge is critical; it runs along the medial face, serving as the attachment site for the interosseous membrane that binds the fibula to the tibia, thereby distributing weight and aiding in load-bearing activities.
The proximal epiphysis of the fibula comprises the fibula head, which articulates with the lateral condyle of the tibia. This articulation is crucial for knee joint stability. The head of the fibula is a key site for the biceps femoris muscle insertion, a component of the hamstrings group. Additionally, the common peroneal nerve wraps around the fibula's neck, just below the head, making it susceptible to injury in this area.
The distal epiphysis extends to form the lateral malleolus, a bony prominence on the outer ankle. It is palpable and more prone to fractures due to its subcutaneous position. The lateral malleolus contributes to the ankle joint stability, providing attachment sites for ligaments such as the anterior talofibular ligament (ATFL) and the posterior talofibular ligament (PTFL), which are critical in preventing excessive inversion and eversion movements of the foot.
The articular surface of the lateral malleolus articulates with the talus and provides a rough surface for the attachment of the distal tibiofibular syndesmosis ligament, further fortifying the ankle joint. Moreover, a recess called the malleolar fossa accepts the attachment of the posterior talo-fibular ligament, and the malleolar groove facilitates the passage of the peroneal tendons, crucial for foot eversion and stability during dynamic movements.
In summary, understanding the detailed anatomy of the fibula and its components is paramount for medical professionals, as it underpins the diagnostic, therapeutic, and rehabilitation processes associated with lower limb injuries. Recognizing the intricate relationship between the fibula and adjacent structures facilitates a holistic approach to managing ankle and lower leg conditions effectively.
Understanding the articulations and ligament attachments of the lower limb is paramount for the comprehensive anatomical and functional comprehension of the human body. This chapter delves into the pivotal aspects of tibiofemoral and tibiofibular articulations, as well as the critical ligament attachments to the tibia and fibula, articulating essential insights for medical students.
The tibiofemoral joint, commonly referred to as the knee joint, is the largest and one of the most complex joints in the human body. It primarily articulates the distal end of the femur with the proximal part of the tibia, enabling pivotal movements such as flexion, extension, and slight medial and lateral rotation. The joint capsule is reinforced by the patella anteriorly and the menisci medially and laterally, providing stability and shock absorption. The articular surfaces of the femoral condyles and the corresponding surfaces on the tibia are covered with hyaline cartilage, reducing friction and facilitating smooth movement. This articulation is secured and stabilized by a network of ligaments, including the anterior and posterior cruciate ligaments, which are critical in maintaining anteroposterior stability.
The tibiofibular syndesmosis, also known as the distal tibiofibular joint, is a slightly movable fibrous joint held together by ligaments. This articulation involves the fibular notch of the tibia and the lateral malleolus of the fibula. It is characterized by the presence of the interosseous membrane, which extends between the interosseous margins of these bones, providing them with stability and distributing weight across the ankle joint. This joint plays a vital role in dissipating axial loads and allowing slight movement between the tibia and fibula during ankle motion, which is crucial for shock absorption and accommodating uneven ground surfaces during locomotion.
Understanding the ligament attachments to the tibia and fibula is fundamental, as these structures play essential roles in the stability and function of the lower limb.
The cruciate ligaments comprise the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL), both of which are key stabilizers of the knee joint. The ACL originates from the anterior intercondylar area of the tibia and extends posteriorly to attach to the medial aspect of the lateral femoral condyle. It plays a crucial role in preventing anterior displacement of the tibia relative to the femur. Conversely, the PCL originates from the posterior intercondylar area of the tibia and extends anteriorly to attach to the lateral aspect of the medial femoral condyle, preventing posterior displacement of the tibia. The unique arrangement of these ligaments in a crossed formation within the joint capsule ensures the knee's stability throughout its range of motion.
The peroneal muscles, comprising the peroneus longus and peroneus brevis, are pivotal lateral stabilizers of the ankle. These muscles originate in the lower two-thirds of the fibula and are secured to the bone through the superficial and deep fasciae of the leg. The peroneus longus extends across the plantar aspect of the foot to insert at the medial cuneiform and the base of the first metatarsal, providing eversion and plantar flexion. The peroneus brevis, on the other hand, inserts onto the base of the fifth metatarsal, facilitating ankle eversion and contributing to ankle stabilization. The close relationship between these muscles and the fibula, alongside their essential functions, underscores the importance of the fibula in lateral leg and foot stability.
In summary, the specific articulations and ligatin attachments involving the tibia and fibula underpin the structural integrity and functional capacity of the lower limb. An in-depth understanding of these complex anatomical configurations is vital for medical students, providing a solid foundation for clinical assessment and management of related conditions.
In the realm of orthopedics and sports medicine, understanding the complexities of the lower leg, especially the malleoli and their propensity for injury, is crucial. This chapter delves into the clinical aspects of fractures and vulnerabilities of the lower leg, techniques for examination and diagnosis, with an emphasis on the medial and lateral malleolus.
The lower leg, characterized by the tibia and fibula, is prone to various injuries, with fractures of the medial and lateral malleoli being among the most common. These injuries are often the result of direct trauma or stress exerted on the ankle joint, making them a frequent concern in emergency and sports medicine.
The medial malleolus, an extension of the distal tibia, is a prominent bone that is crucial for the stability of the ankle joint. Fractures of the medial malleolus typically occur due to excessive force applied to the ankle, such as a severe inversion or eversion injury. Clinically, these fractures present with localized tenderness, swelling, and difficulty in weight-bearing. Medically, understanding the specific type of fracture, whether it be transverse, oblique, or comminuted, is essential for deciding the appropriate treatment plan, which may range from conservative management with immobilization to surgical intervention for more complex fractures.
The lateral malleolus, formed by the distal end of the fibula, is palpable and bears the brunt of lateral ankle stresses. This anatomical structure is particularly vulnerable to fractures, especially due to inversion injuries which cause an abnormal force on the lateral aspect of the ankle. The lower placement of the lateral malleolus compared to the medial malleolus makes it more susceptible to being fractured. These fractures are characterized by pain, swelling, and ecchymosis around the lateral aspect of the ankle. Depending on the severity, treatment may involve conservative management with immobilization or surgical intervention with the aim of restoring the anatomical alignment and stability of the ankle joint.
Proper examination and diagnosis are foundational in the management and treatment of lower leg fractures. This section explores techniques for assessing damage and understanding the implications of associated injuries, such as common peroneal nerve damage.
The initial clinical assessment of suspected malleolar fractures involves a thorough inspection and palpation of the injured area. Observation should focus on identifying signs of deformity, swelling, and skin integrity. Palpation allows for the localization of tenderness and assessment of swelling, which may indicate the presence of a fracture. Additionally, palpating the entire length of the fibula and tibia is critical to rule out proximal injuries. This examination should be gentle to prevent exacerbating the patient's discomfort and must include comparison with the uninjured limb for baseline abnormalities.
The proximity of the fibular neck to the common peroneal nerve presents a risk for nerve damage in cases of fibular fractures. The common peroneal nerve, which wraps around the fibular neck, can be injured during a fracture or subsequent swelling, leading to motor and sensory deficits in the lower leg, such as foot drop or numbness along the lateral shin and dorsum of the foot. A clinical examination for nerve injury includes testing muscle strength, especially the muscles responsible for dorsiflexion and eversion of the foot, and assessing sensory function in the nerve's distribution area. Recognition of nerve injury is crucial, as it significantly impacts the management strategy and prognosis of the injury.
In this chapter, we've explored the clinical intricacies of examining, diagnosing, and understanding fractures and vulnerabilities of the lower leg, with an emphasis on the medial and lateral malleoli. The complexity of these injuries requires a meticulous approach to ensure accurate diagnosis and optimal treatment outcomes.
As we reach the conclusion of our detailed examination of the calf’s skeletal structures, it is crucial to encapsulate the intricate anatomy and biomechanical functions of the tibia and fibula. This recapitulation serves not just as a summary but as a consolidation of understanding for medical students, reinforcing the fundamental aspects of these critical lower limb bones.
The tibia, known for its strength and weight-bearing capacity, is a pivotal component of the lower leg’s skeletal anatomy. Its structure can be delineated into a body and two epiphyses, with the medial placement rendering the tibia a principal supporter in the bipedal stance and locomotion. The superior epiphysis of the tibia is notable for its two articular surfaces that correspond to the femoral condyles, their interaction forming the knee joint. The proximal tibia is marked by the intercondylar eminence, serving as the attachment point for crucial ligaments of the knee. Further, the tibial tuberosity provides a critical insertion site for the patellar ligament, a key player in knee extension.
The distal part of the tibia articulates with the talus bone of the foot through its inferior articular surface, contributing to the ankle joint’s functionality. The prominence of the medial malleolus, extending to articulate with the talus, not only accentuates the medial stability of the ankle but is also a common site for fracture and injury, underscoring the necessity of understanding its anatomy and palpation for diagnostic accuracy.
Parallel to the tibia, the fibula, though not a primary weight-bearing bone, plays a substantial role in the stability of the lower leg and ankle. It is more slender and prismatic, characterized by its twisted nature which facilitates muscle attachment. The fibula’s head articulates with the lateral side of the tibia and aids in the stabilization of the knee joint, whereas its distal part ends in the lateral malleolus—a critical structure for ankle joint stability and prone to fractures, especially in rotational injuries.
The anatomical configuration of the tibia and fibula is instrumental in their biomechanical roles—supporting body weight, enabling movement, and providing leverage and stability. The tibia’s robust structure directly supports the mechanics of walking, running, and jumping by transferring weights, stresses, and forces from the upper body and femur to the ankle and foot. Simultaneously, the fibula, through its ligamentous connections and muscle attachments, contributes to the lateral stability of the ankle and aids in force distribution during various activities.
Understanding the calf’s skeletal anatomy extends beyond its static roles. The dynamic contribution of these bones to movement and posture, their interaction within the musculoskeletal system, and their susceptibility to injury underlines the importance of their study in medical education. This awareness is essential not only in diagnosing and treating lower limb injuries but also in the development of surgical interventions, rehabilitation techniques, and prosthetics design, improving patient outcomes in orthopedic practice.
Through this comprehensive exploration of the tibia and fibula, we aim to equip future physicians with the knowledge and analytical skills necessary to excel in the medical field, particularly in areas involving the musculoskeletal system of the lower limbs. This understanding will no doubt contribute to their competence in clinical settings, enhancing their ability to diagnose, manage, and treat conditions with precision and care.
Articular Facet: A smooth, flat area on a bone, usually covered with cartilage, where it forms a joint with another bone.
Biceps Femoris: A muscle of the thigh located to the back, which causes flexion at the knee.
Condyle: A round prominence at the end of a bone, most often part of a joint - an articular surface.
Dorsiflexion & Plantarflexion: Dorsiflexion refers to the action of depressing the foot (lifting the foot towards the shin). Plantarflexion is the motion of pointing the foot downwards.
Epiphysis: The rounded end of a long bone, at its joint with adjacent bone(s).
Fibula: The smaller of the two bones in the lower leg, lateral to the tibia.
Intercondylar Eminence: A bony structure on the tibial plateau, comprising medial and lateral tubercles.
Interosseous Membrane: A fibrous membrane that connects the tibia and fibula, providing added stability to the lower leg.
Malleolus: The bony prominence on each side of the human ankle - medial (tibia) and lateral (fibula).
Medial & Lateral: Medial is towards the middle of the body. Lateral is away from the middle of the body.
Peroneal Muscles: Muscles located on the outer edge of the lower leg, responsible for plantar flexion and evert the foot.
Popliteus Muscle: A small muscle located at the back of the knee joint, unlocking the knee by rotating the femur on the tibia.
Soleus Muscle: A powerful muscle in the back part of the lower leg (the calf), involved in standing and walking.
Talus: A bone in the ankle that transfers the weight and forces from the shin to the foot.
Tibia: The larger, stronger, and anterior of the two bones in the leg below the knee in vertebrates; it supports most of the weight of the body.
Tibial Tuberosity: A large oblong elevation on the anterior, proximal portion of the tibia, where the patellar ligament attaches.
The text provides an extensive exploration into the anatomical and functional aspects of the lower leg's skeletal structure, focusing on the tibia and fibula, their comparative anatomy, joint articulations, ligament attachments, and clinical relevance. It highlights the tibia as the second longest bone in the human body, essential for weight-bearing and movement, featuring an S-shaped curvature for structural integrity and distributing stresses. The tibia's proximal and distal ends form critical joints at the knee and ankle, respectively, while the fibula, though not primarily a weight-bearing bone, stabilizes the ankle and supports lower leg muscles.
Comparative analysis reveals similarities between the leg's and forearm's bone arrangements, showcasing evolutionary and functional parallels. The text delves into the joint articulations, emphasizing the tibiofemoral and tibiofibular syndesmosis and their importance in the lower limb's stability and function. Crucial ligament attachments to these bones, like the anterior and posterior cruciate ligaments in the knee and the attachments for peroneal muscles on the fibula, underscore their role in movement and stability.
Clinical insights address the commonality of medial and lateral malleolus fractures, their diagnosis, treatment strategies, and the importance of understanding nerve injury implications, such as the common peroneal nerve damage. The detailed examination of the calf's skeletal structures culminates in emphasizing the interplay between the anatomical knowledge of the tibia and fibula with their biomechanical roles in supporting body weight, enabling movement, and contributing to stability. Appendices include a glossary and review questions to further aid in the consolidation of knowledge for medical students, highlighting the significance of the lower leg in medical practice and treatment methodologies.
tibia, fibula, lower leg, skeletal anatomy, anatomy, biomechanics, evolution, comparative anatomy, forearm bones, leg bones, interosseous membrane, syndesmosis joint, epiphysis, proximal epiphysis, distal epiphysis, tibiofemoral articulations, tibiofibular syndesmosis, cruciate ligament, peroneal muscles, common peroneal nerve Tibia, Fibula, Lower Leg, Skeletal Anatomy, Biomechanics, Anatomical Synergy, Comparative Anatomy, Leg Bones, Forearm Bones, S-Shaped Curvature, Triangular Prism Shape, Medial Face, Lateral Face, Posterior Face, Anterior Edge, Tibia Crest, Interosseous Edge, Proximal Epiphysis, Distal Epiphysis, Articulation with the Talus, Medial Malleolus, Fibula Head, Lateral Malleolus, Articular Features, Tibiofemoral Articulations, Tibiofibular Syndesmosis, Cruciate Ligament Insertion Sites, Peroneal Muscles, Examination, Diagnosis, Fractures, Vulnerabilities, Common Peroneal Nerve Injuries, Orthopedics, Sports Medicine, Palpation, Force Transmission, Interosseous Membrane, Malleoli, Tibiofemoral JointThe Complexity of the Lower Leg's Skeletal Anatomy: A Comprehensive ExplorationThe Calf I - Skeletal structures0000