Start learning
This comprehensive text provides an in-depth examination of wrist anatomy, pathologies, and clinical considerations essential for medical students and professionals. It begins by detailing the structural anatomy and joint grouping of the wrist, emphasizing the complexity and susceptibility of the wrist to injuries and disorders. The wrist comprises several joints categorized into four main groups: radiocarpal, carpal (intercarpal), carpometacarpal, and intermetacarpal joints, supporting a wide range of movements crucial for daily activities.
The text further explores the evolutionary significance of the wrist in mammals, especially primates, highlighting adaptations to diverse environmental challenges and lifestyle needs. Primates exhibit specialized wrist anatomy tailored for brachiation and object manipulation, with significant evolutionary developments like an intra-articular meniscus, emphasizing the balance between stability, flexibility, and dexterity. Subsequent chapters dissect the carpal bones and ligaments, showcasing their arrangement, connections, and contributions to wrist function. The text clarifies how the proximal and distal rows of carpal bones, along with palmar, dorsal, and radiate carpal ligaments, facilitate complex gliding and rotational movements essential for hand function. Furthermore, discussions on articular capsule and synovial recesses, joint mechanics, and the unique anatomy of the carpometacarpal and intercarpal joints elucidate their roles in stabilizing the wrist and facilitating dynamic hand movements. The thumb’s trapezometacarpal joint, in particular, is highlighted for its extensive range of motion pivotal to hand function. In addressing wrist pathologies and clinical considerations, the text outlines common conditions such as rheumatoid arthritis, ligamentous structure pathologies, and carpal instabilities, emphasizing the importance of anatomy in diagnosis and treatment. Surgical interventions for managing these conditions, including synovectomy and treatment of carpal fractures and dislocations, underscore the necessity of understanding wrist anatomy for successful outcomes. Overall, the text underscores the wrist's anatomical complexity, functional significance, and evolutionary development, stressing the importance of a thorough understanding for medical diagnosis, treatment, and surgical interventions.The wrist is a complex anatomical structure that serves as a bridge between the forearm and the hand, allowing for the intricate and varied movements required for daily activities. Understanding wrist anatomy is vital for medical students, not only because of its mechanical complexity but also due to its susceptibility to injuries and disorders. This chapter delves into the structural anatomy and joint grouping of the wrist, with a detailed examination of the distal radio-ulnar and radio-carpal joints.
The wrist comprises several joints that are grouped into four main categories: the radiocarpal joint, carpal joints (intercarpal joints), carpometacarpal joints, and the intermetacarpal joints. The distinction between these groups highlights the wrist's multipart structure, where the proximal segment (radiocarpal joint) connects the radius to the first row of carpal bones and the distal segment (midcarpal joint) oversees the articulation between the carpal rows. This organization facilitates the wrist's complex range of movements, including flexion, extension, abduction (radial deviation), adduction (ulnar deviation), and circumduction.
The distal radio-ulnar joint (DRUJ) is a pivotal element within wrist anatomy, categorized as a trochoid type joint that facilitates pronation and supination of the forearm. Articular surfaces present on the ulnar head interact with the ulnar notch of the radius and a critical component known as the articular disc, or triangular fibrocartilage. The articular disc not only completes the articulation surfaces but also plays a pivotal role in maintaining their contact and limiting the range of pronation and supination. This joint is stabilized by the articular capsule and the anterior and posterior radioulnar ligaments, with a synovial layer that extends beyond the articular surfaces, occasionally communicating with the synovial membrane of the radiocarpal joint. Understanding the DRUJ's anatomy and mechanics is essential for comprehending forearm movements and for diagnosing and treating related injuries or disorders.
Moving distally, the radio-carpal joint represents the pivotal point of articulation between the forearm and the hand. Classified as an ellipsoidal joint, it facilitates movements such as flexion, extension, and some degree of circumduction. The articulating surfaces of this joint include a receiver cavity on the forearm side (distal radius and articular disc) and an ellipsoidal prominence on the carpal side formed by the scaphoid, lunate, and triquetrum bones. The division of the carpal articular surface of the radius by a crest into scaphoid and lunate facets is a notable feature, with each facet covered in hyaline cartilage for smooth movement. The structural integrity of the radio-carpal joint is maintained by an articular capsule and a complex system of ligaments, including the dorsal and palmar radiocarpal ligaments and the radial and ulnar collateral ligaments. Detailed knowledge of this joint's anatomy is fundamental for understanding wrist function and for the clinical management of its pathology.
In sum, the structural anatomy and joint grouping of the wrist reveal a highly specialized and complex region designed for a wide range of movements. A thorough understanding of the distal radio-ulnar and radio-carpal joints is crucial for medical students preparing to diagnose and treat conditions affecting the wrist.
The evolution of the wrist across different mammalian lineages, especially in primates, provides invaluable insight into the complexities and variabilities of its structure and function. This chapter aims to elucidate the comparative anatomy of the wrist, delve into the phylogenetic history underscoring its development, and discuss the significance of osseous variations such as the bony lunula that highlight the interplay between genetics, function, and evolutionary pressures.
The wrist, or carpus, while serving a fundamental role across mammals in locomotion and manipulation, exhibits a remarkable range of anatomical variations reflective of the evolutionary adaptations to diverse environmental challenges and lifestyle needs. In non-primate mammals, the wrist typically accommodates the demands of locomotive efficiency and strength, with less emphasis on the intricacies of manipulation found in primate wrists. For instance, the rigid structure observed in ungulates optimizes load-bearing and endurance required for long-distance travel.
In contrast, primates exhibit a highly specialized wrist anatomy tailored for a brachiation lifestyle and intricate object manipulation, highlighting a balance between stability, flexibility, and dexterity. Primates, excluding anthropoid apes, retain a more primitive wrist joint allowing for significant movement between the lower extremity of the ulna and the carpus, particularly with the triquetral and pisiform bones. This configuration facilitates brachiation—the arboreal locomotion method involving swinging under branches by the arms—which is evident in the specialized wrist joints of Hominoidea (superfamily including humans and anthropoid apes), distinct for brachiation adaptations.
Anthropoid apes and humans diverge from simpler primates with the development of an intra-articular meniscus, somewhat separating the ulna from the carpus and partially isolating the ulnar styloid process. This evolutionary novum, particular in its manifestation as a bony lunula (os Daubentonii) in the gibbon's wrist joint, marks a crucial adaptation facilitating enhanced wrist mobility and, in humans, complex tool use.
The evolutionary trajectory of the wrist joint within primates can be understood through a phylogenetic lens that reflects not merely a sequence of changes but an adaptation narrative driven by environmental interactions and survival strategies. The variation in wrist anatomy, from the rudimentary to the complex across primates, signifies the evolutionary pressures—ranging from the necessity for locomotive efficiency to the requirement for dexterous manipulation.
Phylogenetic studies illustrate the gradual retreat of the ulna from direct articulation with the carpus, a hallmark adaptation in hominoids that culminates in the human wrist's sophisticated architecture, designed for versatile movement and precision grip. This evolutionary progression underscores the shift from quadrupedalism to bipedalism, accompanied by an increased reliance on tool use and complex hand functions.
Moreover, the development of the intra-articular meniscus, evolving into structures analogous to the bony lunula, demonstrates a phylogenetic effort to optimize wrist function for articulated motion. This optimization, evident in the enhanced wrist flexibility suited for brachiation in apes and manipulative capabilities in humans, marks a significant pivot in the evolutionary narrative, aligning anatomical adaptations with behavioral shifts towards more complex, tool-oriented lifestyles.
Osseous variations in the wrist, particularly the presence of a bony lunula, underscore the complexity of evolutionary developments within the primate wrist joint. The lunula, observed as intrameniscal ossification in gibbons and posited to merge with the triangular articular disc in higher primates, represents an evolutionary artifact reflecting a transitional adaptation that enhances the carpal complex's mobility and stability.
The significance of the bony lunula lies not only in its structural contribution to the wrist joint but also in serving as a phylogenetic marker, indicating a shared evolutionary pathway among primates that diverges with the advent of more refined manipulative capabilities in humans. Its presence, variability, and integration within the wrist joint complex provide clues to the evolutionary pressures and functional demands that have shaped the wrist's anatomy through millions of years of primate evolution.
In the human wrist, variations such as the bony lunula highlight the evolutionary history of adaptation from a primarily brachial to a manipulative functional mode. These variations, while reflecting the broader phylogenetic narrative, also present considerations for clinical practice, as they can influence joint mechanics, susceptibility to injury, and responses to treatment.
Understanding the comparative anatomy and evolution of the wrist, including the significance of osseous variations like the bony lunula, not only enriches our knowledge of human anatomy but also contextualizes the wrist's complexities within an evolutionary framework. This perspective informs both the clinical appreciation of wrist pathologies and the evolutionary underpinnings that have culminated in the wrist's intricate design, optimized for the diverse functionalities that define human manipulation and interaction with the environment.
The anatomy of the wrist comprises a sophisticated structure of bones and ligaments, each playing a crucial role in the stability, movement, and overall function of the hand and forearm. Understanding the precise configuration and interaction of these components is pivotal for medical students aiming to grasp the intricacies of wrist mechanics, identify potential pathologies, and recommend effective treatments. This chapter zeroes in on the carpal bones and ligaments, dissecting their arrangement, connections, and physiological contributions.
The carpus, or wrist, is formed by eight small bones known as carpal bones, arranged in two rows—proximal and distal. The proximal row consists of the scaphoid, lunate, triquetrum, and pisiform bones. These bones act together as a unit and play a critical role in articulating with the radius and ulna bones of the forearm, facilitating wrist movements such as flexion, extension, abduction, and adduction. The distal row includes the trapezium, trapezoid, capitate, and hamate bones. This row is primarily involved in articulating with the bases of the five metacarpal bones of the hand, thus contributing to the wrist's range of motion and providing stability. The arrangement of these bones, connected by interosseous ligaments, allows for complex gliding and rotational movements essential for hand function. Importantly, the first row of carpals also acts as a transitional structure, distributing forces from the hand to the forearm.
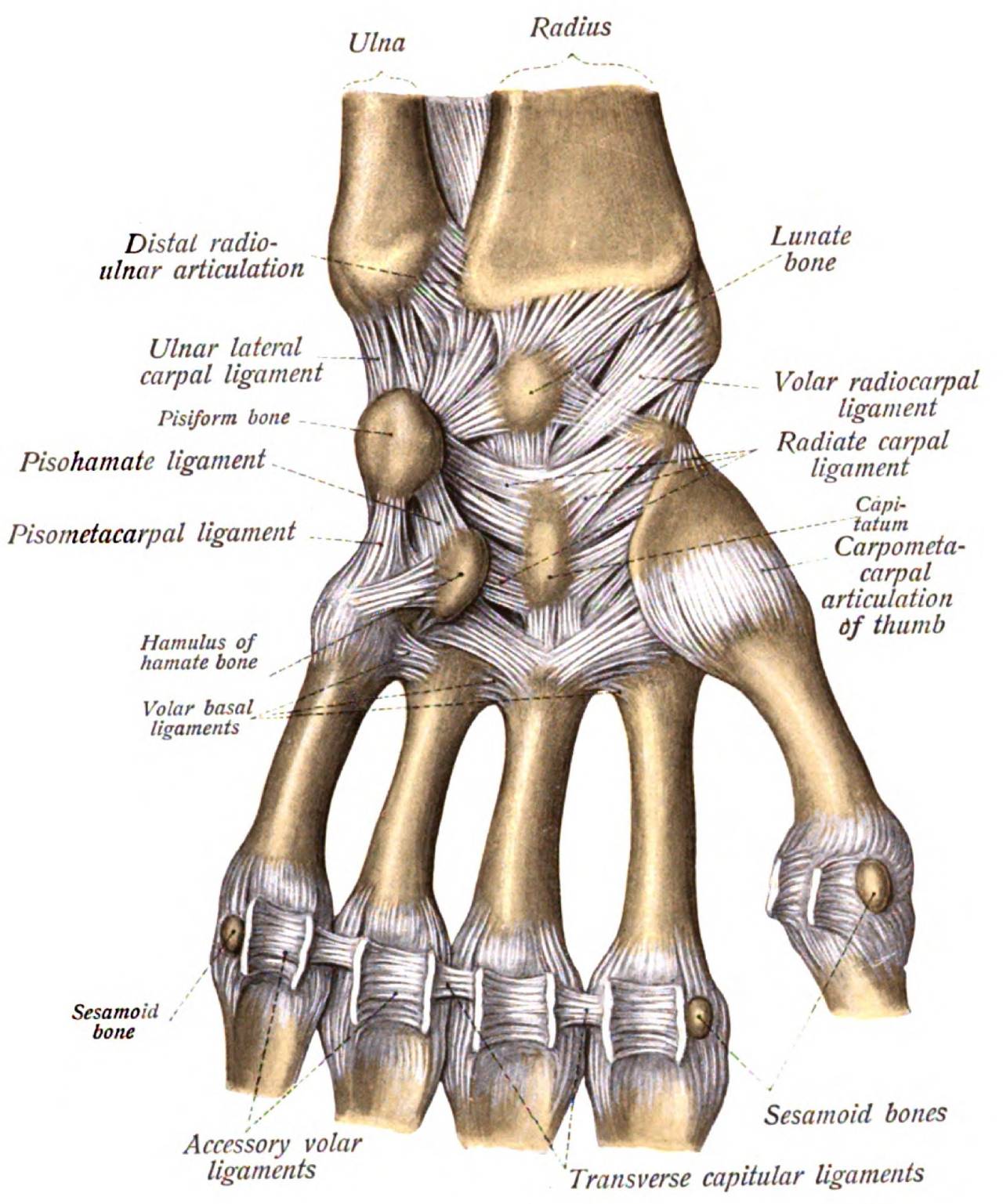
The palmar ligaments of the wrist, comprising the palmar radiocarpal and ulnocarpal ligaments, are integral to the stability and functional integrity of the wrist joint. These V-shaped structures originate from the radius and articular disc, inserting into the carpal bones such as the scaphoid, lunate, and triquetrum, and extending to the "capitate" bone. The palmar radiocarpal ligament strengthens the anterior aspect of the wrist joint, preventing excessive extension, while the ulnocarpal ligament limits radial deviation and supports ulnar-sided structures. These ligaments work in synergy with the dorsal ligaments and the articular capsule to balance the wrist's motion and load distribution, crucial for performing tasks requiring precision and strength.
The dorsal ligaments, though generally considered less robust than their palmar counterparts, serve as vital restraints against extreme volar flexion (palmar flexion) and contribute to the stabilization of the carpal bones. The dorsal radiocarpal ligament extends from the posterior margin of the radius to the dorsal surface of the triquetral bone, creating a tethering effect that balances wrist extension. These dorsal ligaments, along with dorsal intercarpal ligaments, maintain the alignment of the carpal bones and assist in the complex articulation between the two rows of carpal bones, thereby safeguarding against dislocations and facilitating smooth wrist movements.
The radiate carpal ligament, or Lig. carpi radiatum, is a pivotal structure positioned centrally within the wrist. It originates from the capitate bone and radiates outwards in a V-shape to insert into the surrounding carpal bones, particularly the scaphoid and triquetrum/pyramidal. This arrangement allows the radiate carpal ligament to distribute compressive forces across the carpus efficiently, contributing to the wrist's dynamic stability and enhancing the coordination of carpal bone movements. Its strategic placement and robust nature make the radiate carpal ligament essential in maintaining the integrity of the carpal architecture, supporting a wide range of hand functions and movements.
In summary, the carpal bones form a complex network that is paramount for wrist stability and function. The proximal and distal rows of carpal bones articulate with each other and with the bones of the hand and forearm through an intricate system of ligaments, ensuring precise motion and force distribution throughout the upper extremity. A detailed understanding of these anatomical structures and their biomechanical relationships is crucial for diagnosing and managing wrist disorders effectively.
The articular capsule of the wrist joint is a fibrous structure that surrounds the joint and helps to stabilize it. It is reinforced by ligaments and extends beyond the articular surfaces to form a saciform recess that projects upwards to the interosseous space. This extension of the capsule allows for communication with the synovial membrane of the radiocarpal joint, providing a pathway for synovial fluid to move between the two joints.
The prestyloid synovial recess is a consistent anatomical feature of the human wrist joint. It is found near the ulnar styloid process and is associated with the accumulation of blood vessels. This recess varies in size and extends towards the anterior aspect of the ulnar styloid process. In some cases, the ulnar styloid process is covered in articular cartilage and can protrude into the prestyloid recess. This anatomical variation may have clinical significance, as a longer and more robust ulnar styloid process can invaginate the recess and affect joint stability.
Communication pathways between the pisotriquetral and wrist joint cavities have been observed in some individuals. This synovial communication can occur due to deficiencies in the interosseous ligaments, leading to instability in the wrist joint. Additionally, the presence of degenerative changes in the wrist joint, such as perforations of the triangular articular disc, can further affect joint stability. Understanding the anatomy and variations of the articular capsule and synovial recesses is essential for diagnosing and treating wrist joint pathologies.
Understanding the mechanics and movements of joints, particularly the wrist joint, is fundamental for medical students. The wrist is a complex structure that allows a wide range of movements thanks to its intricate anatomy and biomechanics. This chapter delves into the dynamic anatomy of wrist motions, the biomechanics involved in flexion-extension, radio-ulnar deviation, circumduction, and rotational movements.
The wrist's dynamic anatomy enables a wide variety of movements crucial for hand function. The wrist is comprised of several joints, including the distal radio-ulnar joint, the radiocarpal joint, and the midcarpal joint. The distal radio-ulnar joint plays a pivotal role in pronation and supination of the forearm, while the radiocarpal and midcarpal joints allow for the movements of flexion, extension, radial and ulnar deviation, and circumduction.
The articulation between the scaphoid, lunate, and triquetrum with the radius and the articular disc allows the radiocarpal joint to perform flexion and extension. Midcarpal joint movements are facilitated by the articulation between the two rows of carpals, adding nuance to the wrist's range of motion. Ligaments, such as the palmar radiocarpal, palmar ulnocarpal, and dorsal radiocarpal ligaments, as well as the radial and ulnar collateral ligaments, stabilize these movements while allowing flexibility.
Flexion and extension are primary movements at the wrist joint. Flexion inclines the palm towards the forearm's anterior surface (palmar flexion), while extension inclines the back of the hand towards the posterior surface of the forearm (dorsal flexion). These movements occur both in the radiocarpal and midcarpal joints, with the first row of carpals acting as a functional meniscus to facilitate the transition between the forearm and the hand.
Radio-ulnar deviation consists of two movements: radial deviation (abduction) and ulnar deviation (adduction). Radial deviation brings the thumb towards the radius, while ulnar deviation brings the little finger closer to the ulna. These movements are enabled by the distinctive anatomical arrangement of the wrist bones and are limited by the lateral ligaments, which counteract excessive deviation and ensure joint stability.
Circumduction of the wrist is a circular movement that combines flexion, extension, abduction, and adduction. This movement allows the hand to describe a conical space, essential for various hand functions. The unique articulation and ligamentous support system of the wrist facilitate circumduction, ensuring a smooth, coordinated movement.
Rotational movements at the wrist are notably limited due to the wrist's structure. While the wrist itself does not support significant rotation, the proximal and distal radio-ulnar joints allow for the rotational motions of pronation and supination of the forearm. In these movements, the hand does not rotate at the wrist but rather in conjunction with the forearm through the action of the distal and proximal radio-ulnar joints.
In summary, the wrist's complex anatomy allows for a rich repertoire of movements, with each component—bones, joints, ligaments, and articular discs—playing a specific role in facilitating and stabilizing motion. Understanding these mechanisms is crucial for diagnosing and treating wrist conditions effectively, making the study of wrist biomechanics an essential subject for medical students.
The carpometacarpal (CMC) and intercarpal joints represent critical elements in the complex biomechanical apparatus that is the human wrist and hand. These joints allow for the intricate movements necessary for dexterous hand functions, such as grabbing, pinching, and typing. Understanding their anatomy and biomechanics is crucial for medical professionals, especially those specializing in orthopedics, rheumatology, and rehabilitation medicine.
The thumb's carpometacarpal joint, known as the trapezometacarpal joint, is a unique saddle joint that allows for an extensive range of motion, including opposition, reposition, abduction, and adduction. This joint is formed by the articulation between the trapezium bone of the carpus and the first metacarpal bone of the thumb. The articular surfaces of this joint are reciprocally concave and convex, covered with hyaline cartilage, which facilitates smooth movement and provides cushioning against impact.
The anatomical arrangement of the trapezometacarpal joint enables the thumb to perform movements in multiple planes, making it an essential element for hand function. The joint is stabilized by a complex of ligaments, including the anterior and posterior oblique ligaments, the dorsoradial ligament, and the intermetacarpal ligament, which work together to support the thumb during forceful grips and fine manipulative tasks. The articular capsule of this joint is loose, allowing for the wide range of motion necessary for thumb opposition, a movement wherein the thumb moves across the palm to touch the tips of the other fingers.
While the CMC joints of the fingers (digits II-V) do not offer the same range of motion as the thumb, they play a significant role in the stabilization and precise control of hand movements. These joints are primarily plane type joints that permit gliding movements, and they are stabilized by a series of ligaments including the palmar and dorsal carpometacarpal ligaments, and the interosseous ligaments. The palmar carpometacarpal ligaments are particularly important for preventing dorsal dislocation of the metacarpal bones during forceful grips.
These joints contribute to the cupping movement of the hand and the ability to conform to held objects, enhancing grip stability. The biomechanical efficiency of fingers' CMC joints is augmented by their ligamentous structure, which permits a finely tuned balance between mobility and stability, allowing for the transmission of forces from the hand to the forearm with minimal energy loss.
The intermetacarpal joints lie between the bases of the metacarpal bones and are strengthened by the interosseous ligaments. These joints work in sync with the CMC joints to adjust the arching of the hand, an essential component of grip strength and manipulation of objects. The intermetacarpal joints are supported by palmar, dorsal, and interosseous ligaments, which also contribute to the integrity and stability of the hand's structure.
The interosseous ligaments, in particular, play a crucial role in the stabilization of these joints, providing resistance against separation of the metacarpal bones. They also facilitate the transfer of forces across the hand, contributing to the overall dexterity and strength of grip. These ligaments are arranged in a way that allows for slight movement between the metacarpal bones, thus contributing to the flexibility and adaptability of the hand during various tasks.
In summary, the carpometacarpal and intercarpal joints, along with their associated ligaments, allow for the dynamic range of movements and stability necessary for hand function. Understanding the anatomy and biomechanics of these joints is essential for diagnosing and treating disorders affecting the hand and for designing effective rehabilitation strategies to restore hand function following injury.
This chapter delves into the common pathologies affecting the wrist, focusing on rheumatoid arthritis, ligamentous structure pathologies, and carpal instabilities. Understanding these conditions is crucial for diagnosis, treatment, and managing potential complications.
Rheumatoid arthritis (RA) is a chronic inflammatory disorder that primarily affects the joints. In the wrist, RA commonly leads to synovitis, or inflammation of the joint lining, which can result in pain, swelling, and a loss of function. The synovial membrane's proliferation can lead to pannus formation, an abnormal layer of fibrovascular or granulation tissue. This process can erode the articular cartilage and underlying bone, leading to joint deformity.
Anatomically, the wrist's complex structure makes it particularly susceptible to RA's effects. The early symptoms often manifest on the ulnar side of the wrist, significantly impacting the prestyloid recess and the synovial involvement around it. This specific localization of symptoms is thought to be due to the abundant synovial tissue present in these areas, making them prime sites for the inflammatory process of RA.
Management of RA in the wrist requires a comprehensive approach that includes pharmacological treatment to control inflammation and physical therapy to maintain joint function. In some cases, surgical intervention, such as synovectomy, may be necessary to remove inflamed synovial tissue. Understanding the underlying anatomical considerations, such as the role of the prestyloid recess in the pathology of RA, is crucial for effective treatment planning.
The wrist is stabilized by a complex network of ligaments that are subject to various injuries and degenerative changes. Pathologies of these ligamentous structures can arise from acute trauma, chronic overuse, or degenerative diseases, leading to pain, instability, and dysfunction of the wrist.
For instance, tears or sprains of the scapholunate (SL) or lunotriquetral (LT) ligaments can lead to carpal instabilities, which are significant sources of disability. The SL ligament, in particular, is crucial for maintaining carpal alignment and kinematics; its injury can disrupt the intricate motion mechanics between the carpal bones, leading to a scapholunate advanced collapse (SLAC) wrist.
Degenerative changes in the ligaments, such as those seen in older populations or secondary to systemic conditions like RA, can greatly affect wrist stability. The degeneration of the triangular fibrocartilage complex (TFCC), which plays a key role in ulnar-carpal stability, can lead to ulnar impaction syndrome, characterized by ulnar-sided wrist pain, particularly with the forearm in pronation and grip activities.
Early diagnosis through a thorough clinical examination and imaging studies, along with appropriate management strategies including bracing, physical therapy, or surgical repair, is crucial in preventing the progression of these pathologies and preserving wrist function.
Carpal instabilities occur when there is a disruption in the normal kinematic chain of the carpal bones, leading to abnormal motion and potential degeneration of the joint surfaces. These instabilities can be classified based on the direction of instability (dorsal, volar, or dynamic) and the involved carpal bones (for example, scapholunate or lunotriquetral).
Mechanically, the instability usually stems from ligament laxity or tears, particularly of the intrinsic ligaments like the scapholunate or lunotriquetral ligaments, which play pivotal roles in stabilizing specific carpal bone relationships. The loss of these normal relationships can lead to aberrant load transmission across the wrist, resulting in pain, decreased grip strength, and eventual osteoarthritis.
Clinical recognition of carpal instabilities involves a detailed patient history, understanding the mechanism of injury, physical examination highlighting specific maneuvers to elicit pain or demonstrate instability, and imaging. Imaging techniques such as MRI or wrist arthroscopy can offer detailed insights into the integrity of the carpal ligaments and the extent of instability.
Treatment options vary depending on the type and severity of instability, ranging from conservative management with splinting and occupational therapy to restore function and strength, to surgical interventions aiming to reconstruct or repair the damaged ligaments. The surgical approach is often dictated by the specific ligaments involved and the degree of instability.
Understanding the biomechanical implications of carpal instabilities, alongside a thorough anatomical knowledge of the wrist's ligamentous structures, is fundamental for clinicians to devise effective management strategies. Such knowledge ensures that interventions, whether conservative or surgical, are tailored to restore the delicate balance of carpal kinematics, thereby optimizing patient outcomes.
This comprehensive text provides an in-depth examination of wrist anatomy, pathologies, and clinical considerations essential for medical students and professionals. It begins by detailing the structural anatomy and joint grouping of the wrist, emphasizing the complexity and susceptibility of the wrist to injuries and disorders. The wrist comprises several joints categorized into four main groups: radiocarpal, carpal (intercarpal), carpometacarpal, and intermetacarpal joints, supporting a wide range of movements crucial for daily activities.
The text further explores the evolutionary significance of the wrist in mammals, especially primates, highlighting adaptations to diverse environmental challenges and lifestyle needs. Primates exhibit specialized wrist anatomy tailored for brachiation and object manipulation, with significant evolutionary developments like an intra-articular meniscus, emphasizing the balance between stability, flexibility, and dexterity. Subsequent chapters dissect the carpal bones and ligaments, showcasing their arrangement, connections, and contributions to wrist function. The text clarifies how the proximal and distal rows of carpal bones, along with palmar, dorsal, and radiate carpal ligaments, facilitate complex gliding and rotational movements essential for hand function. Furthermore, discussions on articular capsule and synovial recesses, joint mechanics, and the unique anatomy of the carpometacarpal and intercarpal joints elucidate their roles in stabilizing the wrist and facilitating dynamic hand movements. The thumb’s trapezometacarpal joint, in particular, is highlighted for its extensive range of motion pivotal to hand function. In addressing wrist pathologies and clinical considerations, the text outlines common conditions such as rheumatoid arthritis, ligamentous structure pathologies, and carpal instabilities, emphasizing the importance of anatomy in diagnosis and treatment. Surgical interventions for managing these conditions, including synovectomy and treatment of carpal fractures and dislocations, underscore the necessity of understanding wrist anatomy for successful outcomes. Overall, the text underscores the wrist's anatomical complexity, functional significance, and evolutionary development, stressing the importance of a thorough understanding for medical diagnosis, treatment, and surgical interventions.General Overview, Wrist, Anatomy, Medical Students, Injuries, Disorders, Structural Anatomy, Joint Grouping, Radiocarpal Joint, Carpal Joints, Carpometacarpal Joints, Intercarpal Joints, Distal Radio-Ulnar Joint, Forearm Movements, Radio-Carpal Joint, Flexion, Extension, Abduction, Adduction, Circumduction, Comparative Anatomy, Evolution, Mammals, Primates, Wrist Evolution, Phylogeny, Bony Lunula, Osseous Variations, primate wrist, Hand Function, Carpal Bones, Ligaments, Proximal Row, Distal Row, Palmar Ligaments, Dorsal Ligaments, Radiate Carpal Ligament Structure, Articular Capsule, Synovial Recesses, Articular Capsule, Synovial Recess, Prestyloid Synovial Recess, Synovial Communication, Interosseous Ligaments, Joint Mechanics, Wrist Movements, Dynamic Anatomy, Biomechanics, Flexion-Extension, Radio-Ulnar Deviation, Circumduction, Rotational Movements, Wrist Pathologies, Rheumatoid Arthritis, Ligamentous Pathologies, Carpal Instabilities, Surgical Interventions, Synovectomy, Carpal Fractures, Dislocations.Understanding Wrist Anatomy, Pathologies and Surgical InterventionsThe Wrist0000