Start learning
The forearm, comprising two long bones, the ulna and the radius, is critical for daily hand and wrist movements. The ulna, located on the little finger side, forms the elbow joint with its upper processes, the olecranon and the coronoid process, while the radius aligns with the thumb and is essential for wrist joint articulation. Their orientation and articulation, as described in the first chapter, are key to their joint interactions and allow for functional rotational movements, pronation and supination.
The second chapter focuses on the ulna's structure, highlighting its prismatic-triangular shape and importance in arm movement, particularly at the elbow. The anatomy of its body and the proximal and distal ends are thoroughly examined, with emphasis placed on the olecranon and coronoid process at the proximal end, and the head and styloid process at the distal end, which are significant for articulations at the wrist.
The following chapter delves into the radius, lateral in position, and essential for pronation and supination. Similar to the ulna, the radius has a proximal and distal end connected by a body with a distinctive cross-section. The radius's head, neck, and tuberosity are crucial for elbow flexion and forearm supination, while the distal end articulates with wrist bones and has a styloid process that is palpable and important for ligament attachments.
Chapter four discusses the distal radioulnar joint (DRUJ), a synovial pivot joint facilitating forearm rotation. Pathologies of the DRUJ can lead to wrist pain and limited motion, with stability dependent on ligaments and the triangular fibrocartilage complex (TFCC), which is prone to lesions causing dysfunction.
Finally, the fifth chapter covers the clinical and surgical importance of the forearm's anatomy. Surgical approaches to the ulna necessitate an understanding of its complex structure, and various techniques are detailed for internal fixation of ulnar fractures. Special considerations are made for Monteggia fractures and the implementation of precontoured plates to avoid alignment issues.
Overall, these chapters underscore the forearm's essential role in upper limb function, emphasizing the need for a comprehensive anatomical understanding of the ulna and radius for accurate diagnosis and effective surgical intervention.
The forearm represents a complex anatomical structure vital for a multitude of daily activities, including gripping, lifting, and fine motor skills. Understanding the anatomy and function of the forearm bones, namely the ulna and radius, is crucial in the fields of medicine, physiotherapy, and orthopedics. This chapter will delve into the essential aspects of the forearm skeletal structures, elucidating their anatomy, orientation, articulation, and the significance of the interosseous space.
The forearm comprises two long bones, the ulna and the radius, that are positioned parallel to each other and span from the elbow to the wrist. The ulna is situated medially, on the side of the little (pinky) finger, while the radius lies laterally, aligning with the thumb. Structurally, both bones are considered long bones with a middle shaft known as the diaphysis, and ends known as epiphyses.
The orientation of the ulna and radius is paramount to their interaction and joint articulations. At the proximal epiphysis, the ulna extends past the radius, featuring the olecranon process which forms the point of the elbow, palpable under the skin. The intricately shaped trochlear notch of the ulna articulates with the humerus, allowing the elbow to function as a hinge joint. Laterally, the ulna provides a radial notch for the articulation of the radial head, facilitating rotational movements of the forearm known as pronation and supination.
The interosseous space, delimited by each bone's interosseous edge, houses the interosseous membrane, a fibrous sheet connecting the radius and ulna. The significance of this membrane cannot be overstated, as it plays a crucial role in maintaining the parallel alignment of the bones, transmitting forces across the forearm, and serving as an attachment point for various forearm muscles involved in the movements of the hand and wrist.
The ulna is a crucial bone in forearm anatomy, articulating with adjacent structures to facilitate a range of upper limb movements. An understanding of its detailed structure is imperative for medical students, especially those focusing on orthopedics, anatomy, and related surgical fields.
The ulna is a long bone located on the medial aspect of the forearm, playing a central role in arm movement, particularly at the elbow joint. It functions in coordination with the radius to produce supination and pronation, enabling the hand to rotate. The ulna has a prismatic-triangular shape, with a body extending between two widened ends, known as the proximal and distal epiphyses, respectively.
The body of the ulna is the elongated, central part of the bone, which contains areas for muscle attachment and passage of neurovascular elements. It transitions from the larger proximal end to the narrower distal end while maintaining the prismatic profile.
The anterior face of the ulna's body has a nutrient foramen necessary for vascular entry to supply the bone. The upper region serves as the attachment point for the deep flexor muscles of the fingers, while the lower part furnishes attachment for the pronator quadratus muscle - a key player in forearm pronation.
The posterior face features an oblique line, serving as an important muscular attachment site for the anconeus muscle, which assists in elbow extension, and for the ulnar extensor of the wrist, supinator, and thumb and finger extensors that govern movements of the hand and digits.
The medial face of the ulna's body resembles a narrowing strip, palpable under the skin. It supports various muscle insertions and serves as a guide to the anatomical alignment within the forearm.
The anterior edge of the medial face is highlighted by a pronounced ridge extending from the coronoid process to the styloid process. The posterior edge forms a noticeable, subcutaneous S-shaped crest, which is considered when treating forearm injuries or performing surgical interventions.
The lateral or interosseous edge is dedicated to the insertion of the interosseous membrane, a fibrous sheet joining the ulna to the radius. A key feature of this edge is its bifurcation near the radial notch, which accommodates articulation with the radius.
This widened end of the ulna comprises the olecranon and coronoid process, forming a joint with the humerus. This configuration permits a hinge-like movement at the elbow.
The olecranon is the proximal prominence palpable at the elbow, where the triceps brachii muscle inserts, providing leverage for forearm extension. The coronoid process serves as an anchor for the brachialis muscle and creates part of the trochlear notch, which articulates with the humerus.
Just below the coronoid process lies the ulnar tuberosity, marking the site of the brachialis muscle insertion. It plays a role in stabilizing the elbow joint and assisting in flexion movements.
The distal end of the ulna maintains wrist articulation and mirrors the structural intricacy characteristic of the proximal end, ensuring stability and a range of motion at the wrist joint.
The distal ulna terminates with two unique landmarks: the head and the styloid process. The head articulates with the corresponding notch on the radius, aiding in the wrist's complex movements. The styloid process serves as an attachment point for ligaments of the wrist, providing stabilization. Its prominence is palpable under the skin and assists in forming the distal radioulnar joint that enables forearm rotation.
The radius, one of the two principal bones composing the forearm structure, is situated laterally when the body is in the standard anatomical position. It is pivotal for wrist and forearm movements, contributing significantly to pronation and supination. The bone has two ends—proximal and distal—connected by a cylindrical shaft, known as the body. Each end, or epiphysis, has distinctive features contributing to various articulations, facilitating the unique range of movement attributed to the forearm.
The shaft of the radius is characterized by three surfaces and three borders, giving it a triangular cross-section more pronounced towards the distal end. It offers areas for muscular attachments and participates in forming the interosseous space together with the ulna.
The anterior face of the radius features a nutrient foramen, which is vital for bone vascularization. It serves as an attachment site for the flexor pollicis longus muscle, contributing to thumb movement, and for the pronator quadratus muscle, facilitating forearm pronation. Due to its position and function, the anterior face plays a central role in the rotational and flexion movements of the forearm and wrist.
On the posterior aspect, the supinator muscle originates, a key muscle for forearm supination. It also sees the attachment of muscles involved in thumb movements, reinforcing the complexity and versatility of the forearm's functional anatomy. The lateral face of the radius presents a pronator tuberosity for the insertion of the pronator teres muscle. It is partially encased by the supinator muscle, with the deep branch of the radial nerve winding its way around this muscle, highlighting the close relationship between the osseous and neurovascular structures.
The proximal end of the radius is integral in the proximal radioulnar joint, facilitating rotation of the forearm. This epiphysis comprises several anatomical features that are key to its function and stability.
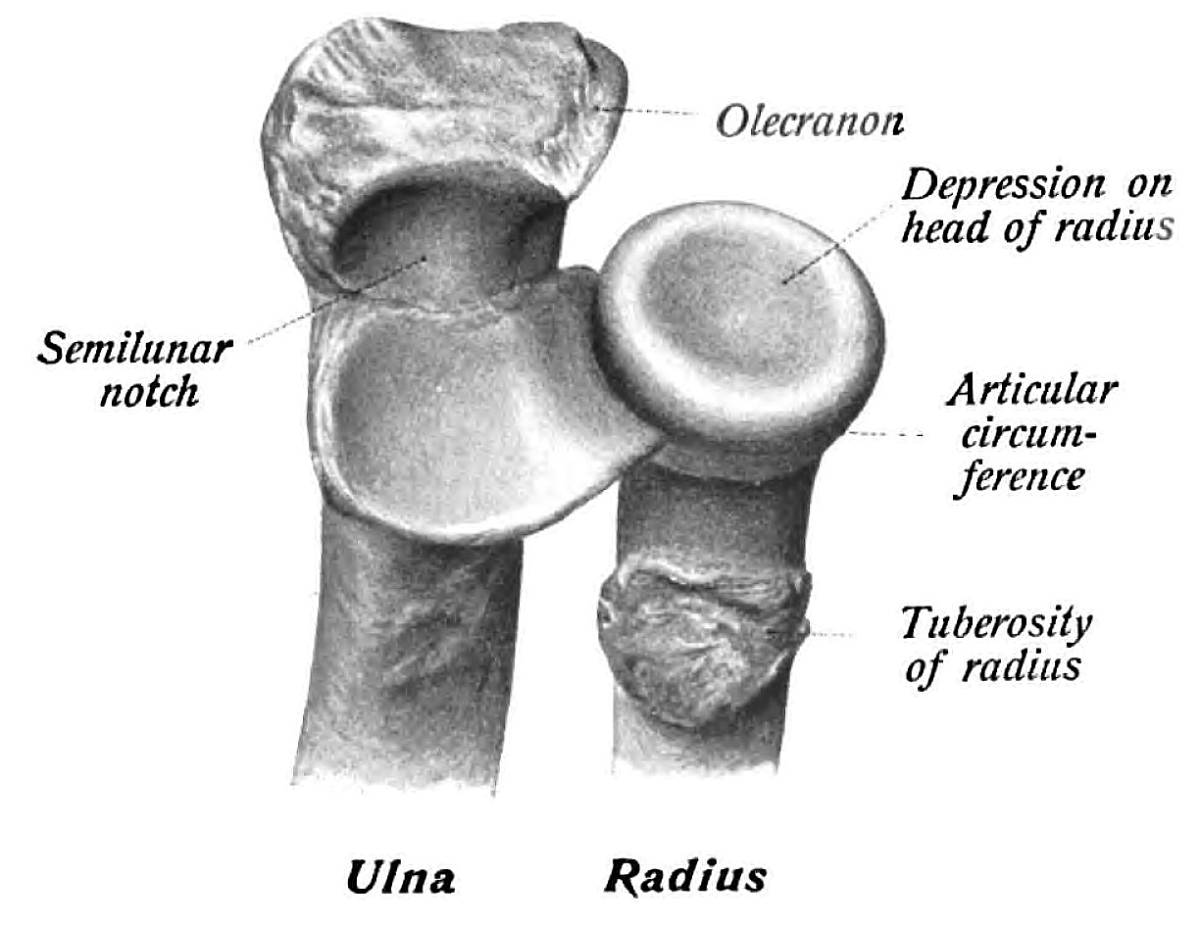
The head of the radius, a disk-like structure, articulates with the capitulum of the humerus at the elbow, and with the radial notch of the ulna, incorporating itself into the proximal radioulnar joint's articulation. The neck forms a slender area separating the head from the tuberosity, which is the bicipital tuberosity—a bony prominence indicative of the biceps brachii muscle's attachment. This arrangement allows for the significant leverage required for flexion at the elbow and supination of the forearm.
The distal end of the radius plays an essential role in wrist joint articulation, capable of exploring through palpation due to its proximity to the skin.
The distal radius bears significant articulating surfaces facilitating the joint's movement. Its lateral aspect forms the ulnar notch that articulates with the distal ulna. The styloid process marks the most distal projection and bears importance for ligament attachments, particularly for ligaments supporting the wrist joint. This process is palpable and extends beyond the ulnar styloid process, offering an external landmark.
The base of the distal radius is designed to articulate with the carpal bones, presenting two distinctive facets divided by a ridge for the scaphoid and lunate bones. These facets are particularly relevant for wrist flexion and extension, as well as radial and ulnar deviation movements. They play an integral role in the composite actions of the hand and emphasize the need for preserving joint integrity during clinical interventions in this region.
The distal radioulnar joint (DRUJ) is a synovial pivot joint that plays a vital role in the complex rotational movement of the forearm, allowing for the motions of pronation and supination. This joint consists of the articulation between the distal end of the radius and the ulna, with the ulnar head and sigmoid notch of the radius forming its primary bony landmarks. The integrity of the DRUJ is crucial for the functionality of the hand, as it contributes to both anteroposterior stability and load transfer across the wrist. During forearm rotation, the radius pivots around the relatively static ulna. The joint's distinct articulation and the congruence between the reciprocal shapes of the distal radius and ulnar head are essential to its stability and smooth motion.
Pathologies of the DRUJ can lead to symptomatic presentations such as wrist pain, limited range of motion, and functional impairment. Injuries can be acute, resulting from trauma such as falls, or chronic, stemming from repeated stress or degenerative diseases like rheumatoid arthritis. Instabilities and pathologies of the DRUJ are clinically significant as they can disrupt the mechanics of the hand and wrist, leading to decreased grip strength and dexterity. DRUJ disorders include subluxations, dislocations, and arthritis, each potentially leading to altered joint mechanics and subsequent compensatory issues in other joints of the upper limb.
The DRUJ anatomy is known to exhibit individual variability, which can affect the functionality and predispose to conditions of instability or reduced range of motion. Variations in the bone contours, such as ulnar length and the shape of the sigmoid notch, can influence the kinematics of the joint. For instance, a negative correlation exists between ulnar length and the mid-coronal length of the sigmoid notch, while ulnar variance is correlated with the obliquity of the DRUJ. Such anatomical differences must be carefully assessed, as they may dictate the personalized approach to treatment and the choice of surgical techniques.
The radioulnar ligaments, located on the dorsal and palmar sides of the joint, are integral components of the TFCC. They are the major stabilizing factor of the DRUJ, with the palmar radioulnar ligament being taut during pronation and the dorsal radioulnar ligament during supination. The TFCC itself includes the articular disc, the meniscus homologue, and various ligamentous structures that extend from the distal radius to the base of the ulnar styloid and the fovea. The complex provides a gliding surface across the DRUJ during forearm movements and serves as a cushion for forces transmitted through the wrist.
Lesions of the TFCC are some of the most common causes of DRUJ dysfunction, often leading to conditions such as ulnar impaction syndrome and instability. The foveal attachment of the TFCC is a critical component of the ligamentous stability of the DRUJ. A foveal detachment or injury can lead to a significant decrease in the DRUJ's stabilizing capacity. TFCC lesions can manifest as a continuum of injury, from minor fraying to complete tears, and the resulting instability can alter the mechanics of the wrist, contribute to ulnar variance, and impair the overall function of the hand. Treatment of TFCC injuries may involve both nonoperative measures, such as wrist splinting and physical therapy, as well as surgical interventions in more severe cases.
The anatomy of the forearm, and in particular the structures of the ulna and radius, have critical clinical implications, especially from the surgical perspective. Understanding the detailed skeletal anatomy of the forearm is indispensable for clinicians to effectively diagnose, manage, and treat pathologies, injuries, and for the successful execution of surgical interventions. Let's delve further into some specific areas of interest:
The posterior border of the ulna serves as a key landmark for surgical approaches targeting the dorsal aspect of the forearm. Surgical intervention on the dorsal surface is often necessary for the reduction and internal fixation of displaced comminuted fractures. The surgeon must carefully navigate the posterior ulnar border to avoid damage to surrounding anatomical structures, such as the ulnar nerve. A thorough understanding of the presence of any radial or undefined bowing in the proximal ulna will further inform the optimal placement of hardware during open reduction internal fixation (ORIF) procedures.
The proximal ulna displays significant anatomical variance. The mean point of varus angulation—clinically essential for the correct placement of internal fixation devices—is positioned approximately 85.4 mm distal to the olecranon. The angulation angle averages 17.7° which can impact the orientation and fitting of orthopedic hardware. Noting these variations is crucial for preoperative planning and ensuring the appropriate technique is applied during surgical intervention.
The anatomical characteristics of the proximal ulna, specifically the shaft width and relationship between its borders, remain critical considerations when selecting the method and devices for internal fixation. Whether using dorsal plates, tension band wiring, or intramedullary screws, each device must accommodate the unique aspects of the ulnar anatomy to ensure stable fixation and facilitate optimal rehabilitation.
Intramedullary screw fixation is especially useful for transverse olecranon fractures or post-osteotomy scenarios, as it offers sufficient cortical bone engagement at the point of varus angulation. However, the application of this technique necessitates accurate knowledge of the proximal ulnar geometry to ensure effective load-bearing and prevent hardware failure.
The advent of angle-stable and contoured plates has significantly enhanced the capacity to achieve fixation of ulnar fractures without the necessity for anatomical bending of the plates. This advancement is particularly beneficial given the complex shape of the proximal ulna. Surgeons must be adept at applying these plates to conform to the varying anatomical landscapes for optimal fracture stabilization.
Monteggia fractures necessitate not only the precise reconstruction of the ulna but also careful attention to the radial head's reduction and stability. The intervention should aim to restore the anatomical alignment of both the ulna and the radius to ensure congruent joint mechanics and avoid long-term complications such as chronic instability or arthritic changes.
The introduction of precontoured plates has improved post-surgical outcomes by mitigating alignment problems. However, given the variability in ulnar anatomy and levels of varus angulation, a comprehensive preoperative assessment remains essential. It is pivotal that the selection of hardware accommodates individual anatomical differences, thereby avoiding complications associated with ill-fitting implants.
In conclusion, the intricate anatomy of the radius and ulna presents several challenges within clinical and surgical practice. Detailed anatomical knowledge allows medical professionals to critically evaluate the most appropriate surgical approach, accurately apply internal fixation methods, navigate the complexities of fracture stabilization, and achieve successful operative treatment outcomes. These chapters provide a window into the manifold considerations that healthcare providers must integrate into their care of patients with forearm and elbow pathologies.
The forearm, comprising two long bones, the ulna and the radius, is critical for daily hand and wrist movements. The ulna, located on the little finger side, forms the elbow joint with its upper processes, the olecranon and the coronoid process, while the radius aligns with the thumb and is essential for wrist joint articulation. Their orientation and articulation, as described in the first chapter, are key to their joint interactions and allow for functional rotational movements, pronation and supination.
The second chapter focuses on the ulna's structure, highlighting its prismatic-triangular shape and importance in arm movement, particularly at the elbow. The anatomy of its body and the proximal and distal ends are thoroughly examined, with emphasis placed on the olecranon and coronoid process at the proximal end, and the head and styloid process at the distal end, which are significant for articulations at the wrist.
The following chapter delves into the radius, lateral in position, and essential for pronation and supination. Similar to the ulna, the radius has a proximal and distal end connected by a body with a distinctive cross-section. The radius's head, neck, and tuberosity are crucial for elbow flexion and forearm supination, while the distal end articulates with wrist bones and has a styloid process that is palpable and important for ligament attachments.
Chapter four discusses the distal radioulnar joint (DRUJ), a synovial pivot joint facilitating forearm rotation. Pathologies of the DRUJ can lead to wrist pain and limited motion, with stability dependent on ligaments and the triangular fibrocartilage complex (TFCC), which is prone to lesions causing dysfunction.
Finally, the fifth chapter covers the clinical and surgical importance of the forearm's anatomy. Surgical approaches to the ulna necessitate an understanding of its complex structure, and various techniques are detailed for internal fixation of ulnar fractures. Special considerations are made for Monteggia fractures and the implementation of precontoured plates to avoid alignment issues.
Overall, these chapters underscore the forearm's essential role in upper limb function, emphasizing the need for a comprehensive anatomical understanding of the ulna and radius for accurate diagnosis and effective surgical intervention.
Forearm Skeletal Structures, Anatomy, Ulna, Radius, Medicine, Physiotherapy, Orthopedics, Epiphyses, Diaphysis, Olecranon, Coronoid process, Wrist joint, Interosseous space, Interosseous membrane,Ulna, Medical students, Orthopedics, Anatomy, Structural overview, Anterior face, Posterior face, Medial face, Proximal epiphysis, Olecranon, Coronoid process, Ulnar tuberosity, Distal epiphysis, Ulnar head, Styloid process,Radius, Wrist joint, Forearm movements, Articulation, Supination, Pronation, Proximal epiphysis, Distal epiphysis, Anterior face, Posterior face, Lateral face, Carpal articular face, Styloid process,Distal Radioulnar Joint (DRUJ), Synovial pivot joint, Pathologies, Clinical relevance, Anatomical variations, Stabilizers, Triangular fibrocartilage complex, TFCC, Ulnar impaction syndrome, Instability, Load distribution,Clinical implications, Surgical anatomy, Dorsal side of the ulna, Proximal ulna, Variations, Angulations, Fracture stabilization, Intramedullary screw fixation, Contoured plates, Monteggia fractures, Radial head management, Precontoured plates, Alignment issuesComprehensive Understanding of the Skeletal Anatomy of the Forearm and Its Clinical ImplicationsThe Forearm I - Skeletal structures0000